

TL;DR:
- Relapse is a common part of addiction, occurring in 40 to 60% within the first year.
- Viewing SUD as a chronic condition helps reduce shame and emphasizes ongoing management.
- Support, early warning recognition, and evidence-based strategies are key to sustained recovery.
Relapse affects 40 to 60% of people in recovery from substance use disorder (SUD) within the first year after treatment. That number surprises many people, yet it mirrors the relapse rates seen in chronic conditions like hypertension and asthma. If you or someone you love has experienced a relapse, the most important thing to understand is this: it is not a sign of weakness, and it does not erase progress. This guide walks through what addiction relapse actually is, why it happens, and what practical steps individuals and families in Los Angeles County can take to respond and move forward.
Table of Contents
- Defining addiction relapse: More than a setback
- Why relapse happens: Triggers, risks, and warning signs
- Relapse is not failure: The chronic disease perspective
- What helps: Evidence-based strategies for relapse prevention
- Beyond the statistics: What most guides don’t tell you about relapse
- How Glendora Recovery Center supports lasting recovery
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Relapse is common | Most people experience relapse during recovery, but it does not mean failure. |
| Manage relapse proactively | Recognizing triggers and warning signs can help prevent lasting setbacks. |
| Long-term support matters | Ongoing care, strategies, and family involvement are vital for sustained recovery. |
| Treatment can be adjusted | Relapse signals the need to revisit or modify treatment, not to give up. |
Defining addiction relapse: More than a setback
Many people use the word “relapse” loosely, but understanding its precise meaning matters for recovery. In addiction medicine, a relapse refers to a prolonged return to problematic substance use after a period of abstinence or controlled use. It is distinct from a lapse, which is a brief, transient slip that does not necessarily lead to full-blown substance misuse. According to research, lapses can be mitigated by continuing treatment rather than abandoning it.
This distinction is more than semantic. A person who has one drink after six months of sobriety has experienced a lapse. If that person returns to daily drinking for weeks, that becomes a relapse. Recognizing the difference helps individuals and families respond appropriately without catastrophizing a single slip or minimizing a serious pattern.
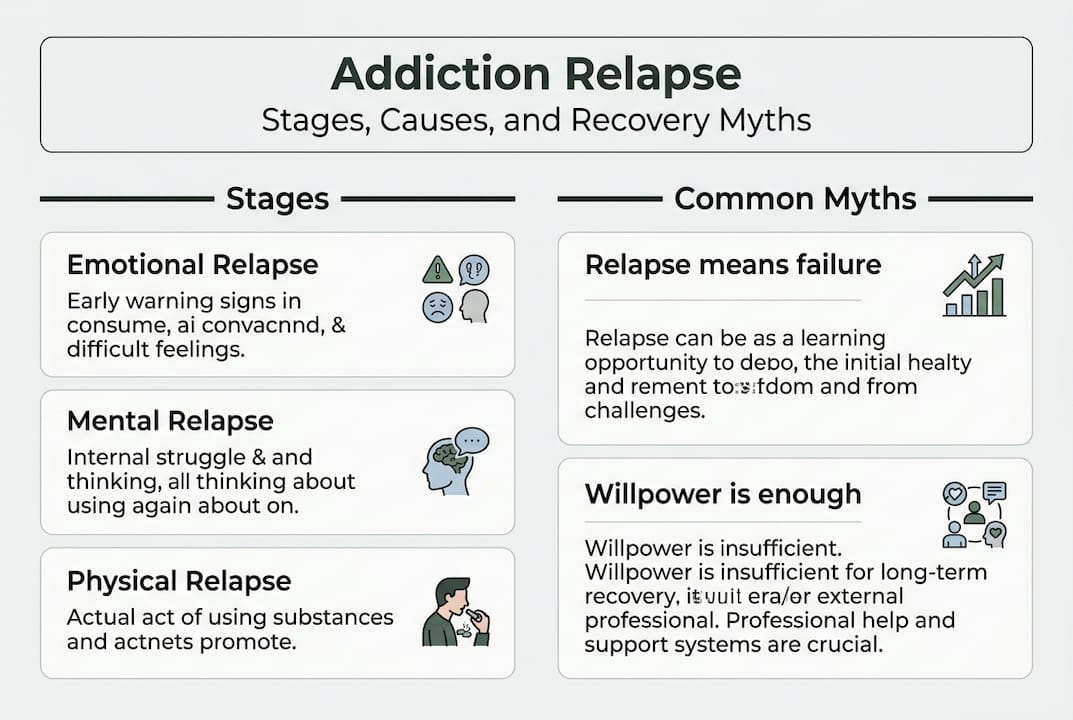
Relapse is also a process, not a single event. It typically unfolds in stages: emotional, mental, and then physical. Emotional relapse can begin weeks before a person picks up a substance again, showing up as isolation, poor self-care, or bottled-up emotions. Mental relapse involves internal conflict, cravings, and bargaining thoughts. Physical relapse is the final stage when substance use resumes.
The medical community views SUD as a chronic condition, much like diabetes or heart disease. Seen through this lens, relapse does not mean treatment has failed. It signals that treatment needs to be resumed, modified, or expanded. This reframing is essential for reducing stigma and encouraging people to seek help rather than hide in shame.
Common misconceptions about relapse include:
- Relapse means the person does not want recovery badly enough
- One relapse erases all previous progress
- People who relapse should start over from scratch
- Relapse is a moral failure rather than a medical event
None of these are accurate. Recognizing the signs of relapse early gives individuals and families the best chance to intervene before a lapse becomes a full relapse.
| Concept | Definition | Clinical implication |
|---|---|---|
| Lapse | Brief, isolated slip in use | Continue treatment; do not abandon recovery plan |
| Relapse | Prolonged return to problematic use | Resume, adjust, or intensify treatment |
| Emotional relapse | Behavioral and mood changes before use | Early intervention opportunity |
| Physical relapse | Actual substance use resumes | Immediate clinical response needed |
“Relapse is not the end of the road. It is a signal that the current treatment plan needs attention, not that recovery is impossible.”
Why relapse happens: Triggers, risks, and warning signs
Relapse does not happen randomly. It follows recognizable patterns driven by biological, psychological, and social factors. Understanding these patterns helps both individuals in recovery and their families stay alert and prepared.
The most common relapse triggers include:
- Stress: Chronic or acute stress activates the same brain pathways involved in addiction, making cravings stronger and impulse control weaker.
- Environmental cues: Returning to places, people, or situations associated with past substance use can spark powerful cravings, even years into recovery.
- Social pressure: Peer pressure or social environments where substance use is normalized can undermine recovery commitments.
- Untreated mental health conditions: Depression, anxiety, PTSD, and other co-occurring disorders significantly increase relapse risk when left unaddressed.
- Overconfidence: Sometimes called “pink cloud syndrome,” feeling too secure in recovery can lead to skipping treatment or support groups.
- Major life changes: Job loss, relationship breakdowns, or grief can destabilize even a well-established recovery routine.
Relapse rates for SUD are 40 to 60% in the first year post-treatment, comparable to hypertension (50 to 70%) and asthma. This comparison is not meant to minimize the challenge but to normalize it. Chronic conditions require ongoing management, and SUD is no different.
For families and loved ones, knowing the early warning signs can make a meaningful difference. Watch for:
- Withdrawal from social activities or support groups
- Increased secrecy or defensiveness
- Romanticizing past substance use
- Skipping therapy or medication appointments
- Mood swings, irritability, or emotional flatness
Genetic factors, age at first use, trauma history, and the presence of co-occurring disorders all influence individual relapse risk. Younger individuals and those with a family history of addiction tend to face higher risk. None of this is about blame. It reflects the biology of recovery and underscores why managing triggers is a skill that requires practice and support.

Pro Tip: Encourage your loved one to write down their personal triggers and share them with their treatment team. Having a written plan for high-risk situations dramatically reduces the chance of a lapse escalating into a full relapse. The importance of support networks cannot be overstated here. Isolation is one of the most consistent predictors of relapse, and connection is one of the most consistent protectors against it. Recognizing relapse warning signs early gives everyone involved a head start.
Relapse is not failure: The chronic disease perspective
One of the most powerful shifts in addiction science over the past few decades is the recognition that SUD is a chronic brain disorder, not a choice or a character flaw. This changes everything about how we interpret relapse.
Consider how we treat other chronic conditions. A person with diabetes who experiences a blood sugar spike does not get told they have failed. Their doctor adjusts their medication, reviews their diet, and modifies their care plan. The same logic applies to addiction. Viewing SUD as chronic means understanding that ongoing management is the goal, not a one-time cure, and that multiple relapses before sustained recovery are common.
| Condition | Relapse/recurrence rate | Ongoing management required |
|---|---|---|
| Substance use disorder | 40 to 60% | Yes |
| Hypertension | 50 to 70% | Yes |
| Asthma | 50 to 70% | Yes |
| Type 2 diabetes | 30 to 50% | Yes |
This comparison is not meant to minimize the seriousness of addiction. It is meant to reduce the shame that prevents people from seeking help after a relapse. Shame is one of the most dangerous emotions in recovery. It drives secrecy, delays treatment, and worsens outcomes.
“Sustained recovery is possible. Most people who struggle with addiction eventually achieve it, often after multiple treatment episodes.”
For individuals and families, adopting the chronic disease model means building recovery into everyday life rather than treating it as a temporary phase. Here are practical steps to implement this mindset:
- Schedule regular check-ins with a counselor or treatment team, even during stable periods.
- Create a written relapse prevention plan that outlines triggers, warning signs, and agreed-upon responses.
- Involve family members in therapy sessions so everyone understands their role in the recovery environment.
- Adjust treatment as needed rather than stopping it when things feel better.
- Celebrate milestones without assuming the work is done.
Exploring chronic care models for dual diagnosis conditions offers a useful framework for understanding how integrated, long-term treatment works in practice.
What helps: Evidence-based strategies for relapse prevention
Knowing that relapse is common and medically understandable is helpful. Knowing what actually prevents it is essential. Research consistently points to several strategies that reduce relapse risk and support long-term recovery.
Cognitive Behavioral Therapy (CBT) is one of the most studied and effective approaches. It helps individuals identify distorted thinking patterns, build coping skills, and rehearse responses to high-risk situations. CBT teaches people to recognize the thought patterns that lead toward substance use before those thoughts translate into action.
Contingency management uses positive reinforcement to reward abstinence and healthy behaviors. It is particularly effective for stimulant and opioid use disorders and can be integrated into outpatient treatment programs.
Medication-assisted treatment (MAT) uses FDA-approved medications such as naltrexone, buprenorphine, and methadone to reduce cravings and withdrawal symptoms. Evidence-based prevention methods including CBT, contingency management, and MAT work best when combined rather than used in isolation.
Additional strategies that support relapse prevention include:
- Building and maintaining a strong social support network
- Practicing consistent self-care: sleep, nutrition, and physical activity
- Identifying and actively avoiding personal triggers
- Attending support groups for recovery such as AA, NA, or SMART Recovery
- Continuing professional treatment even when things feel stable
Pro Tip: Recovery is not just about avoiding substances. It is about building a life that feels worth staying sober for. Focus on lifestyle changes for recovery that bring genuine meaning, connection, and purpose. This makes sobriety sustainable rather than just effortful.
Families play a critical role in this process. Encouraging loved ones to follow through on treatment, reducing shame-based conversations, and participating in family therapy all contribute to better outcomes. Explore relapse prevention strategies and staying sober tips to build a practical toolkit for everyday recovery.
Beyond the statistics: What most guides don’t tell you about relapse
Statistics and strategies are valuable, but they can only tell part of the story. Here is what we at Glendora Recovery Center have observed working with individuals and families across Los Angeles County: the response to relapse matters far more than the relapse itself.
Most recovery journeys include setbacks. The people who achieve lasting sobriety are not the ones who never slip. They are the ones who reach out quickly, without shame, and adjust their approach. Shame and secrecy are the real enemies of recovery. When people feel too embarrassed to tell their counselor or family about a lapse, that silence creates space for a full relapse to take hold.
Family involvement is powerful, but it works best when paired with self-compassion. Loved ones who respond to relapse with anger or ultimatums often push the person further into isolation. A calmer, solution-focused response, supported by peer support networks, tends to produce better results. Recovery is not a straight line. Progress, not perfection, is the goal worth celebrating.
How Glendora Recovery Center supports lasting recovery
At Glendora Recovery Center, we understand that relapse is part of the recovery journey for many people, and we are here to help at every stage. Our programs, including Partial Hospitalization, Intensive Outpatient, and aftercare support, are designed to adjust with your needs over time. We offer individualized care for adults and teens, with flexible scheduling including morning, evening, weekend, and telehealth sessions. Whether you are navigating a recent relapse or working to prevent one, our experienced team can help you build a plan that works. Explore our treatment options or read our lasting recovery guide to learn more. When you are ready, speak with a recovery specialist in a confidential conversation.
Frequently asked questions
Is relapse common in addiction recovery?
Yes, relapse rates for SUD are approximately 40 to 60% in the first year, similar to other chronic illnesses like hypertension and asthma. This makes relapse a medically expected part of the recovery process for many people.
What is the difference between a lapse and a relapse?
A lapse is a brief, one-time slip, while a relapse is a prolonged return to problematic use. Lapses can often be addressed by continuing or adjusting treatment before they escalate.
Does relapse mean addiction treatment has failed?
No. Relapse signals that treatment should be resumed, modified, or supplemented with new support, not that recovery is impossible or that past efforts were wasted.
How can families help after a relapse?
Families can support recovery by encouraging a return to treatment, reducing shame-based responses, participating in family therapy, and creating a stable, supportive home environment that reinforces healthy habits.
What are proven ways to prevent addiction relapse?
CBT, medication-assisted treatment, contingency management, evidence-based prevention strategies, strong support networks, self-care, and consistent trigger avoidance are all proven approaches to reducing relapse risk.
Recommended
- Signs an Addict Is Relapsing – What Families Should Know | Glendora Recovery Center
- Teenage Addiction: Risks, Recovery, and Family Impact | Glendora Recovery Center
- Addiction Recovery Process Explained: Pathways to Healing | Glendora Recovery Center
- Why Ongoing Recovery Matters in Addiction Treatment | Glendora Recovery Center
- Role of Therapy in Trauma Recovery: Evidence and Impact – ReviveHealthTherapy


